Protocols for the prevention and treatment of aging: which methods are preferable?
The topic of correcting age-related changes in the periorbital zone is quite extensive, in particular, with the help of hyaluronic acid fillers. Let us understand the anatomical rationale for the injection of fillers based on hyaluronic acid using the one point technique.
RESTORATION OF THE MIDDLE THIRD OF THE FACE WITH THE ONE POINT TECHNIQUE
The desire to eliminate or at least soften the appearance of dark circles and depressions under the eyes is one of the most common reasons for turning to a cosmetologist, among patients of all ages. The mechanisms of occurrence of these aesthetic defects largely depend on the features of the anatomical structure of the infraorbital region and the patterns of its age-related evolution.
ANATOMICAL FEATURES OF THE INTRAORBITAL AREA
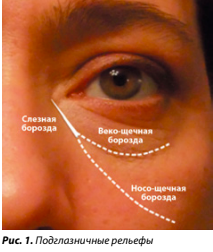
Infraorbital reliefs are determined by the predominance of the eyelid-buccal groove, corresponding to the projection of the orbicular retaining ligament, or the naso-buccal groove, corresponding to the projection of the zygomaticocutaneous ligament, or approximately the same severity of both grooves. In all cases, the most noticeable is the medial component, common to both grooves and designated as the nasolacrimal groove (Fig. 1). In this zone, the orbicularis oculi muscle is firmly attached to the bone using the orbicularis retinaculum ligament [1].
Another important structural component that determines the relief of the medial part of the cheek and infraorbital region is the superficial and deep fatty compartments. According to Rohrich RJ and Pessa JE (2007) [2], the superficial fat packets include nasolabial and malar fat, which in turn consists of the medial and median buccal compartments. The deep fat compartments are represented by the lateral and medial infraorbital fat pads (SOOF), as well as the deep medial buccal fat pad, which is well described in the work
Gierloff M. et al. (2012) [3] based on computed tomography data of unfixed cadaveric material. The boundary between deep and superficial fatty structures is the muscular aponeurotic system (SMAS) and the associated facial muscles.
One of the earliest and most noticeable signs of structural aging of the face is increased contouring of the eyelid-buccal and/or naso-buccal grooves, a general flattening of the centromedial part of the face, and overhang of the nasolabial fold. These changes are based on the processes of stretching and ptosis of the ligamentous apparatus, as well as volumetric changes in the fatty compartments. Indeed, according to Gierloff M. et al. (2012) [3], with age, the distance between the cheek fat packets and the lower orbital margin increases, and the anteroposterior size of the fat compartments becomes thicker in the lower pole and thinner in the upper pole, that is, fat is redistributed under the influence of gravity. The simultaneously occurring decrease in the volume of the deep medial buccal fat pad forms a characteristic clinical picture of the age-related evolution of this area of the face. An analysis of photographs of the same people taken at intervals of several decades (on average 25 years) [4] shows that with age, the shadow from enlarged intraorbital fat pads lengthens the apparent height of the eyelid and visually enhances the existing depth of the tear trough.
yes. In addition, as we age, the skin of the lower eyelid becomes thinner and darker, which also increases the contrast at the border between the eyelid and cheek.
As mentioned above, the nasolacrimal groove region is rigidly fixed in the medial part by the orbicular retinaculum ligament (ORL) [1], limiting the possibility of inferior eyelid displacement. Interestingly, the skin in the upper part of the cheek also practically does not move downwards with age, and the contours in the medial area of the middle third of the cheek change not so much due to ptosis, but due to the evolution of the volume of fatty compartments in the anteroposterior direction. If the skin of the cheek sagged with age, one would expect a change in the direction of the lateral wrinkles of the corners of the eyes with a circular displacement downward. However, this does not happen. In addition, analysis of photographs of the faces of people with any scars or neoplasms in this area also do not demonstrate a clear shift with age [4].
The volume of subcutaneous adipose tissue of the face can vary significantly in patients of different body types, decreasing with age in asthenic individuals and significantly increasing in obesity. However, deep fat packs, which are the structural basis of the face, gradually lose their volume as we age. An anatomical study [5] of the volume and weight of the deep fat compartments of the midface, conducted in 40 cadavers, showed that the average weight of the deep fat compartments was significantly lower in patients older
75 years compared to younger people (1.48 vs 3.41 g, p < 0.001) and 2 times less than the weight of superficial fat (0.2 vs 0.44 g, p < 0.001). Subjects with a body mass index (BMI) less than 20 also had a significant reduction in the magnitude of the ratio between the weight of the deep and superficial compartments (0.15 vs 0.3 g).
These data support the theory of selective atrophy of deep fat pads in the medial midface that occurs with aging or weight loss. That's why
Restoring the volume of these particular structures seems to be a priority for obtaining natural results of facial rejuvenation.
METHODS AND TECHNIQUES FOR CORRECTION WITH FILLERS
When choosing methods and techniques for correction with fillers, one should take into account the anatomical and topographical features of this zone - in the form of the passage of large arterial and venous trunks and nerves (facial and angular arteries and veins, infraorbital neurovascular bundle). This causes an increased risk of trauma to the neurovascular endings when using a needle, as well as ischemic complications. Therefore, many experts consider it preferable to use blunt-ended cannulas for filler injection in the middle third of the face [6].
Foreign literature provides several proprietary methods for restoring the volume of the middle third of the face using a cannula. In particular, in 2010, the work of Cattin TA was published [7], which proposed a method for correcting the middle third of the face using a filler based on stabilized HA through a cannula with single-point access, but the injection level was recommended to be subdermal. The access point for inserting the cannula is selected in the area of the most prominent part of the cheekbone in such a way as to be able to distribute the filler in the area of greatest visual volume loss in the middle third of the face. Conventionally, in the figure, this area is marked with a circle and is located at the intersection of the Hinderer line and a line drawn from the corner of the eye to the corner of the mouth (Fig. 2). On one side of the face, the author suggests introducing from 0.5 to 2 ml of filler using a cannula with a diameter of 18 G and a length of 70 mm.
This correction option should give an immediate good aesthetic result, be quite simple to perform and safe from the point of view of vascular risks. On the other hand, the introduction of a sufficiently large amount of filler into the highly hydrophilic superficial fatty compartments of the infraorbital region is fraught with the formation of persistent edema. In addition, there is a risk of the filler migrating downward over time under the influence of the zygomatic muscles and gravity, especially when introducing sufficiently large volumes of the drug.
Another fairly well-known cannula technique for restoring facial volumes, proposed by BeutJ., is described in detail and anatomically substantiated in the publication by Surek C., BeutJ. et al. (2015)
[8]. Its peculiarity is that the filler based on hyaluronic acid is proposed to be injected deeply supraperiostally, placing it not along the existing grooves and differences in relief, but perpendicular to them (Fig. 3). This option includes Beuth techniques 1, 2 and 3:
- Beut 1: smoothing of the nasolacrimal trough and volumization of superficial nasolabial fat. In this case, the filler is introduced in larger quantities at the starting point with a decrease in volume towards the end. Thus, each pass is shaped like a stalagmite.
- Beut 2: smoothing of the eyelid-buccal groove and reducing the vertical size of the lower eyelid. Small oblique lines of filler are placed along the orbital rim, starting from the space between the orbital septum and the orbitomalar ligament and ending below, in the area of the upper edge of the prezygomatic space.
- Beut 3: volumization of the zygomatic region. Only the latter, the Beuth 4 technique, involves subcutaneous injection of a small amount of filler perpendicular to the nasobuccal groove and Langer's lines.
This is a very interesting and beautiful technique, but it requires some skill development and a very accurate assessment of the required volumes for each injection of the drug. In addition, three cannula approaches from different sides are offered to correct the entire middle third. Finally, the approach for correction according to Beuth 1 has some safety features, since it involves puncturing the skin with a needle in the projection of the possible passage of the facial artery and inserting a cannula in the direction of the infraorbital foramen, which can lead to injury to the vessels and nerves emerging from it.
The third publication that I would like to mention was published quite recently, in 2018, and describes lipofilling of the middle third of the face using a cannula from a single insertion point. This technique was called by the authors “boomerang lifting” [9], as it involves the sequential filling of three deep fat compartments with autologous fat: the medial and lateral SOOF, as well as
the medial buccal fat pad. The relative position of these fat packets resembles a boomerang, which was the reason for the name of this technique (Fig. 4). In this technique, all three fat bags are filled using a cannula from one point located at the intersection of a vertical line drawn along the medial edge of the iris and a horizontal line drawn at the level of the middle of the nasal wing. The medial and lateral SOOF are filled first, followed by the deep medial fat pad. The total volume of injected fat is about 10 ml.
Based on its anatomical basis and the results obtained, this technique seems to be the most interesting and less traumatic and can be modified for the introduction of not only auto-
fat, but also fillers based on hyaluronic acid.
CORRECTION WITH ONE POINT TECHNIQUE
To correct the volume deficit of the middle third of the face using a cannula, you can use a fairly simple but effective technique, which echoes
The same as those described above. It is low-traumatic, as it involves treating the entire area on each side of the face from just one point (that’s why the technique got its name). In this case, the filler is injected supraperiostally into the area of the medial and lateral SOOF, the deep medial fat pad, as well as the prezygomatic space (Fig. 5).
The access point is determined at the intersection of the route of the naso-buccal groove and the line connecting the tip of the eyebrow and the corner of the mouth. In this case, you should first mark the lower edge of the zygomatic arch as a line running from the middle of the wing of the nose to the base of the tragus. This is necessary in order to be sure that the point of puncture of the skin for insertion of the cannula is
is located above the zygomatic arch. This access point is located away from the routes of blood vessels and nerves passing through this area of the face, so the risk of damage to them is relatively small.
At the first stage of the procedure, the naso-buccal sulcus is filled, the total volume of injected filler is about 0.2 ml. Then the cannula is turned perpendicular to the wing of the nose and inserted into the deep medial buccal fat pad, where another 0.2–0.3 ml of the drug is injected as a bolus. The filler should be injected carefully and slowly, monitoring the volume and distributing it in the given area.
When the injection is carried out correctly, not only the restoration of volume in this area becomes noticeable, but also some straightening of the upper third of the nasolabial fold due to a decrease in the degree of its overhang. Finally, at the third stage, the cannula is rotated almost 180° and the zygomatic area is uniformly and linearly filled with 0.5–0.6 ml of filler. Thus, the optimal volume should be considered 1 ml of the drug on each side.
Since one of the features of the infraorbital zone of the middle third of the face is the hydrophilicity of the superficial fatty tissue and the tendency to edema, the correct choice of the drug is of great importance. For safe and effective correction, preference should be given to a drug with low hydrophilicity, good ductility and elasticity.
The results of correction of the middle third of the face using the one point technique are presented in Figure 6.
This article is part of the special project Injection anti-aging
You can read all the articles on this topic:
SPECIAL PROJECT. Injectable anti-aging
Literature:
Alisa SHAROVA, Ph.D., Russian National Research Medical University named after. N. I. Pirogova (Russia)
Read also
- Post-injection reactions: complications and side effects after mesotherapy
- From redness to anaphylaxis: diagnosis and emergency care for allergic reactions
- Results of "Christmas LION" 2025: when fairy tale meets science
- What does hyaluronic acid provide in skin care?
- In focus: a revolutionary solution for the treatment of all types of hyperpigmentation
- Hypoxia of aging: the role of microcirculation in the pathogenesis of age-related skin changes
- In focus: 4D strategy in skin care for hyperpigmentation
- Zero risk: general principles for preventing complications from chemical peels
- Glycation and skin aging
- 4rest (Forest), company
- Rosacea
- Couperosis
- Angioneurosis
- Peloid therapy
- Waxes for depilation
- Fordyce granules
- Bogomolets Olga
- Microneedle therapy